
Psychiatry, Fraud, and the Case for a Class-Action Lawsuit
羅伯特·惠特克-2022 年 8 月 13 日
去年 6 月,Mad in America 收到通知,喬安娜·蒙克里夫 (Joanna Moncrieff)、馬克·霍洛維茨 (Mark Horowitz) 及其同事將很快發表一篇論文,結論是沒有研究結果支持抑鬱症的低血清素假說,我最初想知道我們是否應該費心去報導在上面。Mad in America 的讀者很清楚,低血清素理論早就被揭穿了,我們網站上的許多文章都在講述這一事實,所以我對 MIA 的其他工作人員打趣說,審查這篇文章就像“打死馬(beating a dead horse)”。
When Mad in America received a notice this past June that Joanna Moncrieff, Mark Horowitz, and colleagues would soon publish a paper concluding that there were no research findings that supported the low-serotonin hypothesis of depression, I initially wondered whether we should bother to report on it. Mad in America readers know well that the low-serotonin theory had long ago been debunked, with numerous articles on our site telling of that fact, and so I quipped to other MIA staff that reviewing the article would be like “beating a dead horse.”
但這就是我們在 Mad in America 的小繭(little cocoon)。對於大多數主流媒體來說,他們的論文取得了驚人的發現。在印刷、廣播和電視中,這篇論文被描述為一個“里程碑式”的發現,一個“遊戲規則的改變者”等等,媒體講述了它如何動搖了關於抗抑鬱藥的公認智慧以及“它們是如何起作用的”。
But such is our little cocoon here at Mad in America. For much of the mainstream media, their paper made for a stunning finding. In print, radio, and television, the paper has been described as a “landmark” finding, as a “game changer” and so forth, the media telling of how it has shaken up accepted wisdom about antidepressants and “how they work.”
我認為這很有趣,因為驚訝的驚嘆聲揭示了媒體在過去幾十年裡對精神病學的報導完全失敗了。他們的驚訝是一種默許,他們已經發布了一段時間的宣傳。
This was rather amusing, I thought, as the exclamations of surprise revealed the media’s utter failure regarding their reporting on psychiatry for the past decades. Their surprise served as a tacit confession that they had been publishing propaganda for some time.
然後,當精神科醫生公開評論這篇論文時,出現了第二個供詞,這確實具有“里程碑式”的重要性。他們的評論承認,在過去的幾十年裡,他們的職業犯了醫療欺詐。我在法律意義上使用該術語。
Then, as psychiatrists publicly commented on the paper, a second confession appeared, this one indeed of “landmark” importance. Their comments serve as an admission that, for the past several decades, their profession committed medical fraud. And I am using that term in its legal sense.
正如 Moncrieff 及其同事所指出的,有很長的研究路線未能找到支持抑鬱症低血清素理論的證據。他們工作的新奇之處在於,他們對這項研究進行了全面審查,查看了已完成的不同“類型”研究,並發現所有研究都未能提供支持該理論的證據。作為回應,英國和美國的一些著名精神病學家將這篇論文斥為舊聞。這是一個樣本:
As Moncrieff and colleagues noted, there is a long line of research that failed to find evidence supporting the low-serotonin theory of depression. What was new about their work was that they performed a comprehensive review of this research, looking at the different “types” of studies that had been done, and finding that all had failed to produce evidence supporting the theory. In response, a number of prominent psychiatrists in the UK and the United States dismissed the paper as old news. Here is a sampling:
來自英國精神科醫生:
From UK psychiatrists:
“這次審查的結果並不令人驚訝。抑鬱症有很多不同的症狀,我認為我沒有遇到過任何嚴肅的科學家或精神病學家認為抑鬱症的所有原因都是由血清素的簡單化學失衡引起的。” ——邁克爾·布盧姆菲爾德,倫敦大學學院 (UCL)
“The findings from this review are really unsurprising. Depression has lots of different symptoms and I don’t think I’ve met any serious scientists or psychiatrists who think that all causes of depression are caused by a simple chemical imbalance in serotonin.” —Michael Bloomfield, University College London (UCL)
“這篇論文沒有提出任何新的發現,只是報告了已經在其他地方發表的結果,而且抑鬱症不是由‘低血清素水平’引起的,這當然不是新聞。”——倫敦大學學院遺傳學研究所的大衛柯蒂斯
“This paper does not present any new findings but just reports results which have been published elsewhere and it is certainly not news that depression is not caused by ‘low serotonin levels.’” —David Curtis, UCL Genetics Institute
來自美國精神科醫生:
From US psychiatrists:
“這裡沒有什麼新鮮事。論文周圍的大驚小怪揭示了人們對精神病學的許多無知。從 1990 年代到現在流行的關於抑鬱症的血清素假說是錯誤的,並且長期以來一直被認為是錯誤的,並且從一開始就從未被證明過。” — Nassir Ghaemi,塔夫茨大學醫學院
“Nothing is new here. And the fuss surrounding the paper reveals much ignorance about psychiatry. The serotonin hypothesis of depression which became popular from the 1990s until now, is false, and has known to be false for a long time, and never was proven to begin with.” —Nassir Ghaemi, Tufts University School of Medicine
“當我為 [我的] 書進行研究時,我正在閱讀我確信 Moncrieff 博士及其同事閱讀的相同研究,這些研究基本上是說沒有血清素缺乏的直接證據。所以這並不是什麼新鮮事。” — Daniel Carlat,Carlat 精神病學報告的出版商
“When I was doing research for [my] book, I was reading the same studies that I am sure that Dr. Moncrieff and colleagues read, which were basically saying that there’s no direct evidence of a serotonin deficiency. So it’s not really new.” —Daniel Carlat, publisher of the Carlat Psychiatry Report
做出這些評論的精神科醫生是正確的。精神病學研究界早就知道,低血清素理論並沒有成功,事實上,該領域很久以前就轉向了關於導致抑鬱症的可能病理的新理論。然而,很容易證明,美國精神病學協會與製藥公司合作,在發現低血清素理論毫無價值之後很久就向公眾宣傳了低血清素理論。由著名醫學院的精神病學教授組成的科學諮詢委員會也簽署了非營利性倡導協會的此類聲明,並以這種方式分享了向公眾講述這種“謊言”的罪責。
The psychiatrists making these comments are correct. The psychiatric research community has long known that the low-serotonin theory didn’t pan out and that, in fact, the field long ago moved on to new theories about the possible pathology that gives rise to depression. Yet, as is easy to show, the American Psychiatric Association, in concert with pharmaceutical companies, promoted the low-serotonin theory to the public long after the low-serotonin theory had been found to be without merit. Scientific advisory councils populated by professors of psychiatry at prestigious medical schools also signed off on such pronouncements by non-profit advocacy associations, and in that manner, share culpability for telling this “falsehood” to the public.
從欺騙公眾的意義上講,這種欺詐性的故事講述起了作用。正如 Moncrieff 及其同事所指出的,近年來的調查發現,85% 到 90% 的公眾認為低血清素是抑鬱症的原因,而抗抑鬱藥有助於解決這種不平衡。
That fraudulent story-telling worked, in the sense of deluding the public. As Moncrieff and colleagues noted, surveys in recent years found that 85% to 90% of the public believed that low serotonin was the cause of depression, and that antidepressants helped fix that imbalance.
這就是集體訴訟的基礎:精神病學界很久以前就知道抑鬱症的低血清素故事還沒有平息,但美國精神病學協會、製藥公司和科學諮詢委員會卻告訴公眾,否則這造成了對這個虛假故事的社會信念。調查證明,數以百萬計的患者對這種謊言採取了行動,並將其融入了他們的自我意識中。
There you have the basis for a class action lawsuit: the psychiatric community long ago knew that the low-serotonin story of depression hadn’t panned out, yet the American Psychiatric Association, pharmaceutical companies, and scientific advisory councils told the public otherwise, and this created a societal belief in that false story. The surveys prove that many millions of patients acted upon that falsehood and incorporated it into their sense of self.
醫療欺詐的法律標準
The Legal Standard for Medical Fraud
第二次世界大戰後,納粹對猶太囚犯和精神病患者的醫學實驗的發現導致了一項原則,在美國被編入法律,即有義務為研究中的志願者提供知情同意。潛在的研究對象需要在他們同意之前被告知研究的風險。
In the wake of World War II, the discovery of Nazi medical experiments on Jewish prisoners and the mentally ill led to the principle, codified in law in the United States, of the duty to provide volunteers in research studies with informed consent. Potential study subjects need to be informed about the risks of a study before they can give consent.
在 1950 年代和 1960 年代,這種知情同意原則被擴展到普通醫療保健。該原則基於個人自主權的概念:個人有權自決。1972 年聯邦法院的一個里程碑式案件Canterbury v. Spence裁定,向患者提供知情同意不僅是一項道德義務,而且是一項法律義務。法庭寫道:
In the 1950s and 1960s, this principle of informed consent was extended to ordinary medical care. The principle is grounded in the concept of personal autonomy: the individual has a right to self-determination. A 1972 landmark case in federal court, Canterbury v. Spence, ruled that providing patients with informed consent was not just an ethical obligation, but a legal one. The court wrote:
“患者的自我決定權塑造了披露義務的界限。只有當患者擁有足夠的信息來做出明智的選擇時,才能行使這一權利。”
“The patient’s right of self-decision shapes the boundaries of the duty to reveal. That right can be exercised only if the patient possesses enough information to enable an intelligent choice.”
法院還規定了評估是否已履行這一法律義務的標準:“一個合理的患者想知道關於所提議的治療以及可能固有或潛在涉及的危險的什麼?”
The court also set forth a standard for assessing whether this legal obligation had been met: “What would a reasonable patient want to know with respect to the proposed therapy and the dangers that may be inherently or potentially involved?”
雖然需要獲得患者知情同意的是醫生或醫療護理人員,但該法律標準明確規定了通過代理向個體醫生提供應披露信息的醫學專業的道德義務。醫學專業必須為醫生提供任何建議治療的風險和益處的最佳核算,並且在與公眾的溝通中,也這樣做。
While it is the physician or medical caregiver who is required to obtain the informed consent of the patient, this legal standard clearly imposes an ethical duty, by proxy, on the medical specialty that provides individual physicians with the information that should be disclosed. The medical specialty must provide physicians with the best possible accounting of the risks and benefits of any proposed therapy, and in its communications to the public, do the same.
疾病的診斷顯然是獲得知情同意的第一步。什麼病需要治療?如果出現的症狀不能導致診斷出已知的病理學,那沒關係——缺乏知識有助於為患者的決策提供信息。如果不理解藥物為什麼起作用,那也沒關係。再一次,缺乏知識有助於告知患者的決策。那時,患者可以專注於建議治療的風險和益處:臨床研究表明了什麼?
The diagnosis of a disease is obviously a first step in obtaining informed consent. What is the illness that needs to be treated? If the presenting symptoms do not lead to a diagnosis with a known pathology, that is okay—the absence of knowledge helps inform the patient’s decision-making. If it isn’t understood why a drug works, that is okay too. Once again, the absence of knowledge helps inform the patient’s decision-making. At that point, the patient can focus on the risks and benefits of the proposed treatment: what have clinical studies shown?
化學失衡的故事在每一步都違反了這些原則。患者被告知他們患有已知的病理,並且抗抑鬱藥修復了該病理。那是一個關於疾病解毒劑的故事,因此是醫學上必要的治療方法。如果患者不服用抗抑鬱藥,他或她可能會繼續患有抑鬱症。
The chemical imbalance story violated those principles at every step. Patients were informed that they had a known pathology, and that an antidepressant fixed that pathology. That was a story of an antidote to a disease, and thus was a medically necessary treatment. If a patient didn’t take the antidepressant, he or she could expect to continue to suffer from depression.
這不僅僅是未能為患者提供做出“知情選擇”所需的信息。相反,從法律的角度來看,這是一個病人被騙的案例。
This isn’t simply a failure to give patients the information needed to make an “informed choice.” Instead, from a legal standpoint, this is a case of a patient being told a lie.
以下是亞利桑那州的一家律師事務所如何描述醫生對患者撒謊的法律後果:
Here is how one Arizona law firm describes the legal consequences for a doctor that lies to a patient:
“如果發生某些違反護理義務的行為,你可以起訴你的醫生撒謊。醫生的護理職責是如實告知您的診斷、治療方案和預後。如果醫生對任何此類信息撒謊,則可能是醫療事故索賠的證據。如果醫生未能提供知情同意的真相,法律將其視為醫療過失,這也可能引發電池訴訟。”
“You can sue your doctor for lying, provided certain breaches of duty of care occur. A doctor’s duty of care is to be truthful about your diagnosis, treatment options, and prognosis. If a doctor has lied about any of this information, it could be proof of a medical malpractice claim. The law considers it medical negligence if a doctor fails to provide the truth for informed consent, which may also bring a battery lawsuit.”
如果行為是由於疏忽造成的,則為醫療事故;醫療電池要求行動是有意識的。以下是華盛頓特區一家律師事務所對醫用電池的描述:
Medical malpractice is the charge if the action was due to negligence; medical battery requires the action to be intentional. Here is how a Washington D.C. law firm describes medical battery:
“當您去看醫生並且他們開出治療或程序時,一個基本要素是您的同意。您有權知道將要對您做什麼,了解手術的風險或潛在副作用,並獲悉任何可供您選擇的替代治療方案。. . 當醫生或其他醫療專業人員侵犯您決定您將接受哪些醫療治療以及您不希望接受哪些醫療治療的權利時,就會發生醫療毆打。”
“When you visit a doctor and they prescribe a treatment or procedure, an essential element is your consent. You have the right to know what will be done to you, to learn the risk or potential side effects of a procedure, and to be informed of any alternative treatment options available to you . . . Medical battery occurs when the doctor or other medical professional violates your right to decide what kinds of medical treatments you will receive and which you do not wish to receive.”
當然,FDA 批准了針對抑鬱症的抗抑鬱藥處方。並且可能是許多個人處方者告訴他們的患者抗抑鬱藥可以解決化學失衡,他們認為這是真的。他們認為他們正在為患者提供“知情同意”。
The FDA, of course, approved the prescribing of antidepressants for depression. And it may be that many individual prescribers who told their patients that antidepressants fixed a chemical imbalance thought that was true. They believed they were providing patients with “informed consent.”
因此,在這個化學失衡故事的例子中,醫療事故和電池可以被理解為不一定源於醫患互動,而是美國精神病學協會向公眾講述了一個虛假的故事。 APA) 和製藥公司故意宣傳這種謊言。在兜售這個故事的非營利性倡導組織的科學顧問委員會任職的學術精神病學家分享了這種集體內疚感。
As such, in this instance of the chemical-imbalance story, the medical malpractice and battery can be understood as not necessarily originating in the doctor-patient interaction, but rather in the telling of a false story to the public by the American Psychiatric Association (APA) and pharmaceutical companies that knowingly promoted this falsehood. The academic psychiatrists that served on the scientific advisory boards of non-profit advocacy organizations that peddled this story share in this collective guilt.
欺詐的踪跡
The Trail of Fraud
眾所周知,抑鬱症的低血清素理論起源於 1960 年代的研究結果,即第一代抗抑鬱藥、三環類藥物和單胺氧化酶抑製劑都阻止了通常被稱為單胺的神經遞質的去除。神經元之間的突觸間隙。這導致研究人員在 1965 年假設單胺缺乏可能是抑鬱症的原因。
As is well-known, the low-serotonin theory of depression had its roots in findings, dating back to the 1960s, that the first generation of antidepressants, tricyclics and monoamine oxidase inhibitors, both prevented the usual removal of neurotransmitters known as monoamines from the synaptic cleft between neurons. This led researchers in the 1965 to hypothesize that a deficit in monamines could be a cause of depression.
一旦提出這個假設,研究人員就會試圖確定抑鬱症患者是否真的患有單胺缺乏症。這是一個接一個負面發現的歷史。
Once this hypothesis was floated, researchers then sought to determine whether if patients with depression actually suffered from a monamine deficiency. It’s a history of one negative finding after another.
早在 1974 年,研究人員就得出結論,迄今為止所有此類研究都表明“大腦去甲腎上腺素、多巴胺或血清素的消耗本身不足以解釋抑鬱症臨床綜合徵的發展。” 這是第一輪調查結果,之後有人猜測單胺缺乏症可能存在於部分抑鬱症患者中(而不是所有此類患者共有的病理學)。1984 年,NIMH進行了一項研究調查這種可能性。再一次,底線調查結果是否定的,這導致 NIMH 研究人員得出結論,“5-羥色胺能係統功能的升高或降低不太可能與抑鬱症有關。”
As early as 1974, researchers concluded that all such studies up to that time indicated that “the depletion of brain norepinephrine, dopamine, or serotonin is in itself not sufficient to account for the development of the clinical syndrome of depression.” This was the first round of findings, and after that there was speculation that a monoamine deficit might be present in a subset of depressed patients (as opposed to being a pathology common to all such patients.) In 1984, the NIMH conducted a study to investigate that possibility. Once more, the bottom-line findings were negative, which led the NIMH researchers to conclude that “elevations or decrements in the functioning of serotonergic systems per are not likely to be associated with depression.”
那時,這個假設已經存在了近 20 年,並且被發現是有缺陷的。在研究界,有一種感覺,即該假設總是對大腦如何運作進行了過度簡化的描述,因此研究未能支持該假設也就不足為奇了。即便如此,在 1984 年的那份報告之後,調查人員繼續研究抑鬱症患者是否患有低血清素,隨著 1988 年百憂解上市後,這項研究加速了。嘗試了許多不同的調查方法,但結果再次是否定的。該假設於 1999 年被美國精神病學協會正式埋葬,當時它出版了第三版精神病學教科書。情緒障礙部分的作者甚至指出了導致抑鬱症化學失衡理論的錯誤邏輯。他們寫:
At that point, the hypothesis had been around for nearly two decades and found to be wanting. In the research community, there was a sense that the hypothesis had always presented an overly reductive picture of how the brain functioned, and thus it wasn’t a surprise that research had failed to support the hypothesis. Even so, after that 1984 report, investigators continued to study whether depressed patients suffered from low serotonin, with this research quickening after Prozac arrived on the market in 1988. Many different investigative methods were tried, but once again, the results were negative. The hypothesis was officially buried by the American Psychiatric Association in 1999, when it published the third edition of its Textbook of Psychiatry. The authors of a section on mood disorders even pointed out the faulty logic that had led to the chemical imbalance theory of depression in the first place. They wrote:
“單胺假說於 1965 年首次提出,認為去甲腎上腺素和 5-HT [血清素] 等單胺缺乏抑鬱症,抗抑鬱藥的作用取決於增加這些單胺的突觸可用性。單胺假說基於抗抑鬱藥阻斷去甲腎上腺素、5-HT 和/或多巴胺的再攝取抑制的觀察。然而,從觀察到的一類藥物對神經遞質可用性的作用推斷神經遞質病理生理學類似於得出結論,因為阿司匹林會導致胃腸道出血,頭痛是由過多的血液引起的,而阿司匹林對頭痛的治療作用涉及失血。其他經驗尚未證實單胺耗竭假設。” 1
“The monoamine hypothesis, which was first proposed in 1965, holds that monoamines such as norepinephrine and 5-HT [serotonin] are deficient in depression and that the action of antidepressants depends on increasing the synaptic availability of these monoamines. The monoamine hypothesis was based on observations that that antidepressants block reuptake inhibition of norepinephrine, 5-HT, and/or dopamine. However, inferring neurotransmitter pathophysiology from an observed action of a class of medications on neurotransmitter availability is similar to concluding that because aspirin causes gastrointestinal bleeding, headaches are caused by too much blood and the therapeutic action of aspirin in headaches involves blood loss. Additional experience has not confirmed the monoamine depletion hypothesis.”1
在接下來的幾年裡,該領域的其他專家也贊同這一點。精神病學家斯蒂芬斯塔爾在他 2000 年出版的教科書《基本精神藥理學》中寫道:“沒有明確和令人信服的證據表明單胺缺乏會導致抑鬱症。也就是說,沒有‘真正的’單胺缺乏。” 2
Other experts in the field echoed this point in the next few years. In his 2000 textbook Essential Psychopharmacology, psychiatrist Stephen Stahl wrote that “there is no clear and convincing evidence that monamine deficiency accounts for depression; that is, there is no ‘real’ monoamine deficit.”2
研究文獻中出現了更多這樣的坦白,最後,在2010 年的一篇論文中,以精神障礙生物學著稱的埃里克·內斯特勒詳細介紹了對低血清素理論的多種類型的調查是如何達成一致的結論:
More such confessions appeared in the research literature, and finally, in a 2010 paper, Eric Nestler, famous for his work on the biology of mental disorders, detailed how the many types of inquiries into the low-serotonin theory had all come to the same conclusion:
“經過十多年的 PET 研究(適合定量測量受體和轉運蛋白的數量和占有率)、單胺耗竭研究(暫時和實驗性地降低大腦單胺水平)以及檢查單胺能基因多態性的遺傳關聯分析,有幾乎沒有證據表明抑鬱症的病理生理學中血清素能、去甲腎上腺素能或多巴胺能神經傳遞的真正缺陷。這並不奇怪,因為沒有先驗理由表明治療的作用機制與疾病的病理生理學相反。”
“After more than a decade of PET studies (positioned aptly to quantitatively measure receptor and transporter numbers and occupancy), monoamine depletion studies (which transiently and experimentally reduce brain monoamine levels), as well as genetic association analyses examining polymorphisms in monoaminergic genes, there is little evidence to implicate true deficits in serotonergic, noradrenergic, or dopaminergic neurotransmission in the pathophysiology of depression. This is not surprising, as there is no a priori reason that the mechanism of action of a treatment is the opposite of disease pathophysiology.”
這就是今天的精神科醫生在被問及對 Moncrieff 的論文發表評論時所指的研究歷史,他們說“這裡沒有什麼新東西”。他們是對的。這個理論很久以前就被拋棄了。在2011 年的博客中,美國精神病學協會的貿易刊物Psychiatric Times的編輯 Ronald Pies是這樣說的:“事實上,‘化學失衡’的概念一直是一種都市傳說——從來沒有一個理論被認真提出過由見多識廣的精神科醫生提供。”
This is the research history that psychiatrists today, when asked to comment about Moncrieff’s paper, are referring to when they state, “there is nothing new here.” They are right. The theory was abandoned long ago. In a 2011 blog, Ronald Pies, editor of Psychiatric Times, the trade publication of the American Psychiatric Association, put it this way: “In truth, the ‘chemical imbalance’ notion was always a kind of urban legend—never a theory seriously propounded by well-informed psychiatrists.”
從法律的角度來看,APA 出版的《精神病學教科書》第三版1999年是這段歷史上的關鍵時刻。直到那個時候,可以提出這樣的論點,即雖然抑鬱症的生物學仍然未知,但一種假設是它是由於血清素水平低,並且仍在努力看看這是否是真的。然而,在那之後,APA、製藥公司和組成科學顧問委員會的學術精神病學家有義務告知公眾,低血清素理論並沒有得到證實。相反,如果這三個群體告訴公眾抑鬱症患者患有可以通過藥物修復的化學失衡,那麼他們就是在故意向公眾撒謊,因此,按照知情同意的標準,他們是在教唆醫療事故和醫療電池的患者。
From a legal standpoint, the APA’s publication of the third edition of its Textbook of Psychiatry in 1999 is the pivotal moment in this history. Up until that time, the argument could be made that while the biology of depression remained unknown, one hypothesis was that it was due to low serotonin, and that there were still efforts to see if that might be true. However, after that date, the APA, the pharmaceutical companies, and the academic psychiatrists that populated the scientific advisory councils had an obligation to inform the public that the low-serotonin theory had not panned out. If instead these three groups informed the public that depressed patients suffered from a chemical imbalance that could be fixed by a drug, they were knowingly telling the public a lie, and thus, by informed consent standards, they were abetting medical malpractice and the medical battery of patients.
很容易證明這正是 APA、製藥公司和科學顧問委員會所做的。
And it’s easy to document that is exactly what the APA, the pharmaceutical companies, and the scientific advisory boards did.
APA 宣傳化學失衡的故事
The APA’s Promotion of the Chemical Imbalance Story
APA對精神障礙化學失衡理論的推廣可以追溯到1980年出版的《診斷與統計手冊》第三版。該出版物經常被描述為美國精神病學的變革時刻,因為當時 APA 採用了一種“疾病”模型來診斷和治療精神疾病。
The APA’s promotion of the chemical imbalance theory of mental disorders can be traced back to 1980, when it published the third edition of its Diagnostic and Statistical Manual. That publication is regularly characterized as a transformative moment for American psychiatry, as this was when the APA adopted a “disease” model for diagnosing and treating psychiatric disorders.
沒有任何科學發現可以促進這種轉變。出現的科學衝動源於DSM II 的失敗:該版本中的診斷被理解為“缺乏可靠性和有效性”。這導致聖路易斯華盛頓大學的一組研究人員主張精神病學應該重新開始:它可以開髮用於對具有相似症狀的患者進行分組的類別,希望隨後的研究能夠“驗證”這些分組是真正的疾病。DSM II將被放棄,並為研究目的製定新的類別。
There were no scientific findings that spurred this transformation. The scientific impulse that was present arose from the failure of DSM II: the diagnoses in that edition were understood to “lack reliability and validity.” That led a team of researchers at Washington University in St. Louis to advocate that psychiatry should start fresh: it could develop categories for grouping patients with like symptoms, with the hope that subsequent research would “validate” the groupings as real diseases. DSM II would be abandoned, and new categories would be drawn up for research purposes.
然而,在 1970 年代,APA 領導人談到,面對各種批評,精神病學如何為生存而戰。其診斷手冊被認為缺乏有效性;心理學家和諮詢師提供的談話療法似乎與精神分析一樣有效;《飛越杜鵑巢》將精神病院的工作人員描述為真正的瘋子;一場“抗精神病學”運動將精神病學描述為一種社會控制機構。
However, during the 1970s, APA leaders spoke of how, in the face of various criticisms, psychiatry was fighting for its survival. Its diagnostic manual was understood to lack validity; psychologists and counselors were offering talk therapies that appeared to be as effective as psychoanalysis; One Flew Over the Cuckoo’s Nest depicted staff in mental hospitals as the truly crazy ones; and an “antipsychiatry” movement described psychiatry as an agency of social control.
最刺痛的批評是精神科醫生不是“真正的醫生”。有一個顯而易見的解決方案在招手:如果他們採用疾病模型,他們可以將自己展示為治療真實疾病的醫生。這將使他們能夠穿上“白大褂”——無論是比喻性的還是字面意義上的——社會公認的“真正”醫生的外衣。
The criticism that stung the most was that psychiatrists were not “real doctors.” There was an obvious solution that beckoned: if they adopted a disease model, they could present themselves as physicians who treated real diseases. This would enable them to don the “white coat”—both figuratively and literally—that society recognized as the garb of “real” doctors.
APA 主席 Jack Weinberg 在 1977 年表示, DSM III將“向任何可能懷疑我們將精神病學視為醫學專業的人澄清”。3
DSM III, said APA president Jack Weinberg in 1977, would “clarify to anyone who may be in doubt that we regard psychiatry as a specialty of medicine.”3
DSM III發布後,APA 開始向公眾推銷其新的疾病模型。1981年,成立“出版營銷處”,“深化精神科醫生的醫學鑑定”。同年,它成立了一家出版社,將“精神病學最優秀的人才和最新知識呈現給大眾閱讀”。它制定了一個全國性的專家名冊來推廣這種疾病模型,並成立了一個“公共事務學院”來舉辦研討會,培訓其成員“處理廣播和電視的技術”。4
Once DSM III was published, the APA set out to market its new disease model to the public. In 1981, it established a “division of publications and marketing” to “deepen the medical identification of psychiatrists.” That same year it established a press to bring “psychiatry’s best talent and current knowledge before the reading public.” It developed a nationwide roster of experts to promote this disease model, and it set up a “public affairs institute” to run workshops that trained its members “in techniques for dealing with radio and television.”4
這項公關工作講述了精神病學的一場革命,媒體告知研究人員正在發現導致精神病症狀的“分子”。APA 舉辦了“媒體日”來促進這種理解,向報導這場革命的媒體頒發獎項,很快報紙和雜誌就開始撰寫有關非凡進步的故事,預示著精神障礙可以“治愈”的一天。
This PR effort told of a revolution in psychiatry, with the media informed that researchers were discovering the very “molecules” that caused psychiatric symptoms. The APA held “media days” to promote this understanding, with awards given to media that reported on this revolution, and soon newspapers and magazines were writing stories about extraordinary advances that heralded a day when mental disorders could be “cured.”
《巴爾的摩太陽報》在 1984 年獲得普利策說明性新聞獎的七部分系列文章中以這種方式描述了這場革命:
The Baltimore Sun, in a seven-part series titled “The Mind-Fixers,” which won a Pulitzer Prize for expository journalism in 1984, described the revolution in this way:
“十多年來,研究精神病學家一直在實驗室里安靜地工作,解剖老鼠和人類的大腦,並梳理出解開心靈秘密的化學公式。現在,在 1980 年代,他們的工作得到了回報。他們正在迅速識別產生人類思想和情感的連鎖分子。. . 因此,今天的精神病學站在了成為一門精確科學的門檻上,就像分子遺傳學一樣精確和可量化。未來是一個心理工程時代,以及專門藥物和療法的發展。” 5
“For a decade and more, research psychiatrists have been working quietly in laboratories, dissecting the brains of mice and men and teasing out the chemical formulas that unlock the secrets of the mind. Now, in the 1980s, their work is paying off. They are rapidly identifying the interlocking molecules that produce human thought and emotion . . . As a result, psychiatry today stands on the threshold of becoming an exact science, as precise and quantifiable as molecular genetics. Ahead lies an era of psychic engineering, and the development of specialized drugs and therapies.”5
當然,製藥公司對 APA 採用疾病模型感到非常興奮,因為他們知道這將極大地擴大他們的藥物市場,因此他們開始向 APA 和學術醫療中心的精神科醫生提供資金以支持這項公關工作.
Pharmaceutical companies, of course, were thrilled with the APA’s adoption of a disease model, for they understood it would greatly expand the market for their drugs, and they began funneling money to the APA and to psychiatrists at academic medical centers to support this PR effort.
本質上,化學失衡的故事是最能向公眾推銷這種疾病模型的原聲。這一主張符合關於 20 世紀醫學發展的更大的社會敘述:胰島素作為糖尿病的治療藥物、抗生素治療傳染病、脊髓灰質炎疫苗等等。現在輪到精神病學在這次遊行中佔據主導地位了。
The chemical imbalance story served, in essence, as the soundbite that could best sell this disease model to the public. It was a claim that fit into a larger societal narrative about the march of medicine in the 20th century: insulin as a treatment for diabetes, antibiotics for infectious diseases, a vaccine for polio, and so forth. Now it was psychiatry’s turn to take its place at the head of this parade.
在DSM III發布後,公眾立即開始聽到這個聲音片段。1981 年,美聯社一篇採訪芝加哥大學精神病學家赫伯特·梅爾策的文章告訴讀者,“研究人員認為臨床抑鬱症是由大腦中的化學物質失衡引起的”,並且已經有兩種藥物正在開發中“恢復化學物質不平衡”恢復正常。6
The public began hearing this soundbite immediately after DSM III was published. In 1981, an Associated Press article featuring an interview with University of Chicago psychiatrist Herbert Meltzer informed readers that “researchers believe clinical depression is caused by a chemical imbalance in the brain,” and that there were already two drugs in development that “restore the chemical imbalance” to normal.6
三年後,即將成為美國精神病學雜誌主編的南希·安德烈森(Nancy Andreasen)出版了一本暢銷書,名為《破碎的大腦:生物革命》。她寫道,對精神病學的新認識是“主要的精神疾病是疾病”,每種“不同的疾病都有不同的具體原因…… . . 有許多跡象表明,精神疾病是由於大腦中的化學物質失衡造成的,而治療涉及糾正這些化學物質失衡。” 7
Three years later, Nancy Andreasen, who would soon become editor-in-chief of the American Journal of Psychiatry, published a best-selling book titled The Broken Brain: The Biological Revolution. The new understanding in psychiatry, she wrote, was that the “major psychiatric illnesses are diseases,” and that each “different illness has a different specific cause . . . there are many hints that mental illness is due to chemical imbalances in their brain and that treatment involves correcting these chemical imbalances.”7
禮來公司於 1988 年將百憂解推向市場,很快公眾就听說這種“選擇性血清素再攝取抑製劑”可將血清素恢復到正常水平,因此就像“治療糖尿病的胰島素”。紐約雜誌在其封面上刊登了這種藥丸:“Bye,Bye Blues”宣佈為標題。8 新聞周刊也做了同樣的事情,藥丸上的標題是:“百憂解,一種治療抑鬱症的突破性藥物。” 9
Eli Lilly brought Prozac to market in 1988, and soon the public was hearing that this “selective serotonin reuptake inhibitor” restored serotonin to normal levels, and thus was like “insulin for diabetes.” New York magazine featured the pill on its cover: “Bye, Bye Blues” declared the headline.8 Newsweek’s did as well, with this headline atop the pill: “Prozac, A Breakthrough Drug for Depression.”9
雜誌和報紙的故事講述了患者的感覺比以往任何時候都好。1990 年春天,《紐約時報》在一篇可以說是美國最著名的科學作家娜塔莉·安吉爾(Natalie Angier )的文章中告訴讀者:“所有抗抑鬱藥的作用都是恢復大腦中神經遞質活動的平衡,糾正控制情緒、思想、食慾、疼痛和其他感覺的電化學信號異常過度或抑制。” 弗朗西斯·蒙迪莫爾博士告訴安吉爾,這種新藥“不像酒精或安定。就像抗生素一樣。”
Magazine and newspaper stories told of how patients were feeling better than ever. In the spring of 1990, the New York Times, in an article by Natalie Angier, who arguably was the nation’s most well-known science writer, informed readers that “all antidepressants work by restoring the balance of neurotransmitter activity in the brain, correcting an abnormal excess or inhibition of the electrochemical signals that control mood, thoughts, appetite, pain, and other sensations.” This new drug, Dr. Francis Mondimore told Angier, “is not like alcohol or Valium. It’s like antibiotics.”
電視節目也傳達了類似的信息,在60 分鐘節目中,萊斯利·斯塔爾講述了一位女性瑪麗亞·羅梅羅(Maria Romero)的鼓舞人心的故事,她在經歷了十年可怕的抑鬱症之後,在百憂解上重生了。“有人,有什麼東西離開了我的身體,另一個人進來了,”羅梅羅說。斯塔爾解釋了正在發揮作用的生物療法:“大多數醫生認為,像羅梅羅這樣的慢性抑鬱症是由大腦中的化學失衡引起的。為了糾正它,醫生開了百憂解。” 10
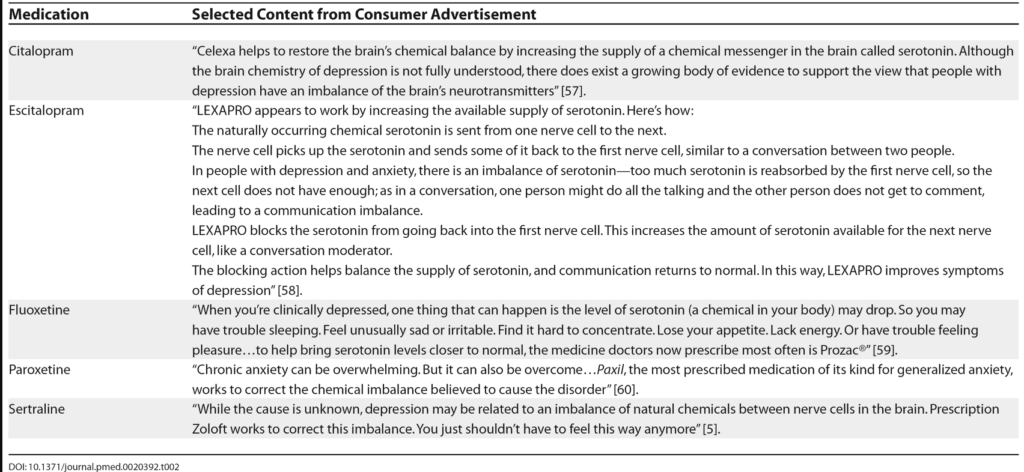
百憂解的銷售額飆升,隨著其他製藥公司將新的“SSRI”抗抑鬱藥(Zoloft、Paxil、Celexa、Lexapro 等)推向市場,他們依靠化學失衡的聲音來推銷他們的產品。全國精神疾病聯盟在此期間聲名鵲起,其核心信息是精神疾病是由大腦化學失衡引起的疾病,而精神藥物可以解決這些失衡問題。
美國民眾和全球民眾開始將這個故事理解為科學真理。新千年到來了,儘管 APA 自己的教科書已經宣布低血清素理論已經死灰復燃,但 APA 公開加倍強調了化學失衡的故事,告訴公眾它現在已經得到證實。
“在過去的十年裡,神經科學和精神病學研究已經開始揭示大腦的秘密,”APA 主席理查德哈丁在 2001 年發表在Family Circle上的一篇文章中寫道。“我們現在知道,精神疾病——比如抑鬱症或精神分裂症——不是‘道德弱點’或‘想像的’,而是由大腦結構異常和大腦化學物質失衡引起的真實疾病。” 11
在同一期中,未來的 APA 主席 Nada Stotland 告訴讀者,抗抑鬱藥“使大腦化學物質恢復正常”。
公眾相信了。2005 年 5 月 4 日,美國心理學會發布新聞稿,慶祝其進行的一項調查發現“75% 的消費者認為精神疾病通常是由大腦中的化學物質失衡引起的”。APA 主席 Steven Sharfstein 表示,這證明了“[公眾] 了解心理健康的好消息”。新聞稿很有幫助地指出,精神科醫生是“經過專門培訓以診斷和治療化學失衡的專家”。
同年,APA 出版了“讓我們談談關於抑鬱症的事實”小冊子,其中傳達了同樣的信息:“可以開抗抑鬱藥來糾正大腦中化學物質水平的不平衡。”
APA 的“公共教育網站”繼續講述未來 16 年的化學失衡。最後,在 2021 年初,羅納德·派斯寫道,他終於設法讓 APA “刪除”該消息。
即便如此,APA 網站仍然向公眾講述了該故事的有限版本。訪問標題為“什麼是抑鬱症”頁面的訪問者了解到,“大腦化學可能會導致個人的抑鬱症,並可能影響他們的治療。出於這個原因,可以開抗抑鬱藥來改變一個人的大腦化學。”
科學顧問委員會
在 1980 年代和 1990 年代,製藥公司和美國精神病學協會意識到,非營利性宣傳組織,如全國精神疾病聯盟,可以幫助他們向公眾推銷他們的疾病模型,並向公眾宣傳治療的有效性。精神科藥物。醫藥資金流向了 NAMI 和其他倡導組織,很快,擔任行業思想領袖的學術精神病學家就加入了非營利性倡導組織的科學諮詢委員會。
在2014 年發表在 Mad in America 上的博客中,Philip Hickey 確定了三個著名的消費者組織,這些組織告知公眾抑鬱症是由化學物質失衡引起的,並公佈了在其科學顧問委員會任職的精神病醫生的姓名。這是列表:
兒童和青少年雙極基金會
- Joseph Biederman,醫學博士,哈佛醫學院精神病學教授
- Gabrielle Carlson,醫學博士,精神病學和兒科教授,Stonybrook 州立大學兒童和青少年精神病學主任
- Kiki Chang, MD, 斯坦福大學兒童和青少年精神病學副教授兼兒科雙相情感障礙項目主任
- Melissa DelBello,醫學博士,辛辛那提大學精神病學和兒科教授
- Robert L. Findling,醫學博士,凱斯西儲大學兒童與青少年精神病學教授
- Janet Wozniak,醫學博士,哈佛醫學院精神病學助理教授
抑鬱症和雙相支持聯盟
- Gregory E. Simon,醫學博士,公共衛生碩士,精神病學家和高級研究員,西雅圖 GroupHealth 研究所
- Michael E. Thase,醫學博士,精神病學教授。匹茲堡大學
- Mark S. Bauer,醫學博士,布朗大學醫學院精神病學副教授
- Joseph R. Calabrese,醫學博士,凱斯西儲大學精神病學教授兼情緒障礙項目主任
- David J. Kupfer,醫學博士,匹茲堡大學精神病學系教授兼主席
- George S. Alexopoulos,醫學博士,康奈爾大學精神病學教授
- Gary Sachs,醫學博士,哈佛大學雙極研究項目主任
- Mark A. Frye,醫學博士,Mayo Clinic 精神病學教授
- J. Raymond DePaulo Jr. MD,約翰霍普金斯大學精神病學教授
- William Beardslee,醫學博士,波士頓兒童醫院首席精神科醫生
納米
- Nancy Andreasen,醫學博士,愛荷華大學醫學院精神病學系主任。
- Ellen Frank 博士,匹茲堡大學醫學院精神病學和心理學教授。
- David Kupfer,醫學博士,匹茲堡大學醫學院精神病學教授和神經科學教授。
- Jeffrey Lieberman,醫學博士,哥倫比亞大學精神病學系主任,紐約州精神病學研究所所長。
- Henry Nasrallah,醫學博士:副院長;辛辛那提大學精神病學和神經科學教授。
- Charles Nemeroff,醫學博士:邁阿密大學衛生系統精神病學和行為科學系主任。
- S. Charles Schulz,醫學博士:明尼蘇達大學醫學院精神病學系教授兼系主任。
名單上的名字構成了當時著名學術精神病學家的“名人錄”,眾所周知,其中許多人因其對行業的“思想領袖”服務而獲得了數十萬美元的報酬。他們是一個集體的聲音,告訴美國公眾抑鬱症是由於化學失衡造成的,可以通過有助於糾正這種失衡的抗抑鬱藥成功治療。在 APA 宣布低血清素理論已死 15 年後,這些網站上的抗抑鬱藥仍然被視為一種疾病的解毒劑。
雖然許多消費者組織現在已經從他們的網站上清除了此類聲明,但它們並沒有完全消失。例如,兒童心理研究所的網站,在標題為“抑鬱症兒童用藥”的頁面上,提供了對抗抑鬱藥的描述:
Child Mind Institute 的創始人是美國最著名的兒童精神病學家之一,Harold Koplewicz。他是紐約大學醫學院兒童和青少年精神病學系主任,自 1997 年以來一直擔任《兒童和青少年精神藥理學雜誌》的主編。他的個人資料頁面指出,兒童精神研究所的主要任務是“通過提供值得信賴的信息和資源來教育和授權父母。”
製藥公司
任何在新千年頭十年看過電視的人都知道,製藥公司利用化學物質失衡的故事來銷售他們的抗抑鬱藥。例如,輝瑞公司的“Sad Blob”廣告充斥著航空公司,如果你密切關注,你會發現輝瑞公司知道化學物質失衡的故事是沒有根據的。然而,無論如何,它還是利用化學故事來銷售其藥物。它用兩個簡短的句子完成了這種口頭上的花招:“雖然(抑鬱症)的原因尚不清楚,但抑鬱症可能與大腦中神經細胞之間的天然大腦化學物質的不平衡有關。左洛復處方可以糾正這種不平衡。”
廣告以這樣的提示結束:“當您對錯誤的了解更多時,您可以幫助糾正錯誤。”
如果律師提起集體訴訟,這就是他們可能提出的欺詐線索。他們可以詳細說明可追溯到 1970 年代的長期研究如何未能發現低血清素是導致抑鬱症的原因。他們可以證明,1999 年 APA 自己的教科書宣布該理論已死並被埋葬。然後他們可以詳細說明 APA、倡導組織的科學顧問委員會和製藥公司在此之後如何繼續推廣化學失衡理論,將抗抑鬱藥作為修復化學失衡的藥物出現。這種持續的宣傳證明,從 1999 年起,這三個群體故意宣傳虛假,患者可能會據此採取行動。
這是大規模實施醫療欺詐的證據——也可以說是社會醫療電池。
化學失衡故事的另一半
雖然研究人員沒有發現被診斷患有抑鬱症的人在服用抗抑鬱藥之前血清素系統異常,但他們確實發現這些化合物首先引發了被假設導致疾病的異常。
SSRI的基本機制是眾所周知的。當突觸前神經元將血清素釋放到神經元之間的微小間隙(稱為突觸)中時,血清素分子與突觸後神經元上的受體結合,然後,一瞬間,血清素從突觸中去除。一種酶代謝少量的血清素;其餘的被迅速泵回突觸前神經元,通過稱為 SERT 的通道進入。在 1975 年的一篇論文中,禮來公司的科學家報告說,氟西汀(一種將作為百憂解上市的化合物)阻斷了這種再攝取過程,導致“血清素在突觸處堆積”。
然而,突觸前神經元的末端膜上有“自身受體”,用於監測突觸中的血清素水平,隨著血清素水平的升高,這些自身受體開始尖叫,正如一位科學家打趣的那樣,“關閉血清素機器”。突觸前神經元開始以較低的速率放電,而突觸後神經元降低其血清素受體的密度。
換句話說,藥物降低了血清素傳遞的加速器,大腦通過踩剎車做出反應。
隨著時間的推移,可能會出現其他變化。有反饋迴路將不同的神經遞質系統相互連接,因此對藥物的這種初始反應可能是一系列尚未確定的下游變化的前奏。然而,對氟西汀的最初反應很早就充實了,它告訴了氟西汀是如何在這個系統中引起嚴重異常的,而不是使血清素能通路正常化。
1996 年,NIMH 主任 Steven Hyman 發表了一篇題為“啟動和適應:理解精神藥物作用的範式”的論文,講述瞭如何理解所有精神藥物會導致大腦功能異常。
他寫道,精神科藥物會“造成神經遞質功能的擾動”。為了應對這種擾動,大腦會經歷一系列補償性適應,在每種情況下,直接的適應是大腦對抗藥物的影響。一種抗精神病藥阻斷了多巴胺的傳遞,作為回應,大腦的多巴胺能通路至少在一段時間內進入高速運轉狀態。抗抑鬱藥會提高突觸中的血清素水平,作為回應,大腦會阻止其血清素能通路。海曼寫道,這些補償性適應“植根於存在的穩態機制,大概是為了讓細胞在面對環境變化或內部環境變化時保持平衡。”
海曼描述了一種被稱為“對立耐受”的適應性變化。他繼續說,一段時間後,這種藥物的“長期給藥”會導致“神經功能發生重大而持久的改變”。作為這一過程的一部分,細胞內信號通路和基因表達會發生變化。幾週後,他得出結論,這個人的大腦以“在質量和數量上都不同於正常狀態”的方式運作。
“在質量上和數量上都不同”。事實上,禮來公司的兩位科學家 Ray Fuller 和 David Wong 很早就觀察到氟西汀,因為它破壞了血清素能通路,可用於研究“血清素神經元在各種大腦功能(行為、睡眠、垂體激素釋放的調節)中的作用” 、疼痛反應等。” 為了進行這樣的實驗,研究人員可以給動物服用氟西汀,以觀察哪些功能受到損害。他們會尋找出現的病狀。
這就是 1990 年代末關於抗抑鬱藥治療抑鬱症的科學知識狀況。沒有證據表明抑鬱症患者在服用抗抑鬱藥之前血清素偏低,但研究表明,一旦他們這樣做了,他們的大腦就會開始以一種“在質量和數量上都不同於正常狀態”的方式運作。
抗抑鬱藥被宣傳為“正常化藥物”,而事實上研究人員知道它們是“異常化”藥物。
傷害完成
在他們對 Moncrieff 論文的回應中,許多精神病學家提出了“沒有傷害,沒有犯規”的論點。“抗抑鬱藥有效,”他們說,因此開抗抑鬱藥是一種有益的做法,即使人們對抑鬱症的原因和藥物的作用存在一些混淆。
以下是馬薩諸塞州精神病學家丹尼爾卡拉特在接受國家公共廣播電台“On Point”節目的採訪時所說的:
“醫生並不確切知道(抗抑鬱藥)是如何起作用的。患者確實想知道那裡有解釋。有時我們確實必須給他們一個速記的解釋,即使它並不完全準確。”
就化學失衡的危害而言,抗抑鬱藥是否能在一段時間內減輕患者的症狀是無關緊要的。化學失衡的故事告訴患者他或她患有腦部病變,需要使用治療該病變的藥物進行治療。這是一個診斷故事,它改變了患者的自我意識和對自己思想的理解。此外,治療旨在改變個人對世界的情感反應方式——這是一種最深刻的干預。
事實上,服用抗抑鬱藥的決定使患者走上了不同的生命歷程。它使一個人走上藥物治療的未來之路,而不是這個人以前知道的生活以及如果他或她尋求其他一些非藥物治療形式的人可能擁有的生活。從這個意義上說,是否服用抗抑鬱藥的決定就像眾所周知的岔路口——兩種不同的生活在前面延伸。
這就是當化學失衡的故事被告知尋求抑鬱症幫助的患者時所造成的傷害:他們根據謊言對自己的未來做出了深刻的決定。
化學失衡的故事也在社會層面造成了傷害。它重塑了我們的集體自我意識。
在百憂解上市之前,NIMH 的一項調查發現,只有 12% 的美國成年人表示他們會服用避孕藥來治療抑鬱症。這項調查告訴公眾,在某種程度上,經歷一段痛苦是正常的,生活有起有落,人們通常可以呼籲內心的複原力和環境支持來領導他們走出了黑暗的隧道。
但隨後出現了精神病學模型的銷售,並且以相當快的順序,公眾開始以新的眼光看待人性:我們的情緒是由一種叫做血清素的分子控制的,如果一個人經歷過抑鬱症,他們有,用話說南希·安德烈森(Nancy Andreasen),“腦殘”。
這一概念也扼殺了創造一個更好地培養心理和情感健康的社會的政治努力。化學物質失衡的故事將抑鬱症的原因置於個人大腦中,這符合新自由主義議程,但對導致痛苦和抑鬱的社會條件視而不見:貧困、無法獲得體面的住房、缺乏兒童保育支持等等上。
正如蒙克里夫所寫,調查發現超過 85% 的公眾開始相信抑鬱症是由低血清素引起的。這個數字說明了一個陰謀——一個公會、製藥公司和學術精神病學家——深刻地背叛了我們的社會。他們告訴我們一個故事,他們自己的研究被證明是錯誤的,他們這樣做是因為這有利於公會利益和製藥公司的經濟利益。至於科學委員會的成員,他們正在簽署一個讓他們作為行業“思想領袖”保持良好聲譽的故事,並進一步提升了他們作為該領域領導者的公眾聲譽。
從法律的角度來看,“抗抑鬱藥是否有效”並不重要。對患者和社會撒謊是一種醫療電池,任何可能的治療益處都不能成為這種欺騙的藉口。然而,當審查“抗抑鬱藥有效”的說法時,可以看出這是這些藥物虛假營銷的延續。
抗抑鬱藥有效嗎?
當公眾被告知一種藥物“有效”時,他們會被引導相信大多數服用該藥物的人可以預期會受益。例如,抗生素是一種可以說“有效”的藥物。當 1940 年代引入青黴素和其他抗生素時,它們治癒了細菌感染和許多細菌疾病:肺炎、猩紅熱、白喉和肺結核,僅舉幾例。但不能說抗抑鬱藥以這種方式起作用。
可以說的是,有一些臨床研究提供了有關短期和長期抗抑鬱藥可能的風險和益處的信息。相關信息可以分為三類。
安慰劑對照試驗
當精神科醫生說抗抑鬱藥“有效”時,他們大多引用了行業資助的藥物試驗結果。這些短期試驗的薈萃分析發現,在52 點漢密爾頓抑鬱評定量表上,藥物治療組和安慰劑組在症狀減輕方面的差異約為2 分。雖然這種差異可能具有統計學意義,但其臨床意義值得懷疑。
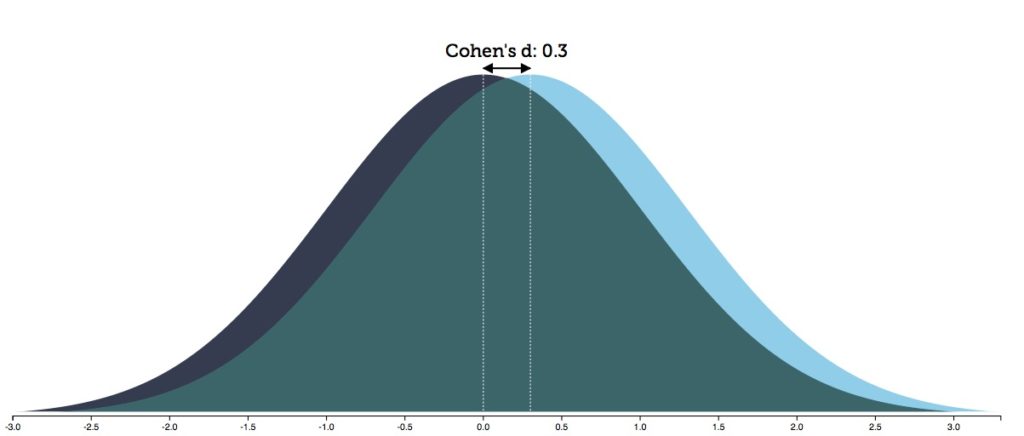
了解這種差異的最佳方法是查看其影響大小。在個人水平上,反應沿著鐘形曲線下降,效應大小的可視化揭示了安慰劑組和藥物治療組的鐘形曲線有何不同。研究人員得出結論,工業試驗中的“效應量”為 0.3(效應量的範圍可以從 0 到 3.0)。
如下圖所示,當治療的效果大小為 0.3 時,兩組的鐘形曲線有 88% 的重疊。這意味著您需要用抗抑鬱藥治療 8 個人,才能多生產一個從治療中受益的人。接受藥物治療的 8 人中有 7 人將暴露於藥物的不良反應,除了安慰劑之外沒有任何額外的好處。
對“真實世界”患者的研究
行業資助的試驗通常在預計最有可能對藥物反應良好(無合併症等)的患者子集中進行,因此被認為不一定反映一般人群的結果。在美國通常由國家心理健康研究所資助的“現實世界”患者研究通常不是安慰劑對照,而是簡單地尋求評估有多少百分比的患者以顯著方式對治療。
這些研究報告的抗抑鬱藥“反應”率低於行業資助的試驗,特別是較差的保持良好率。
在2004 年對 118 名接受抗抑鬱藥治療的真實世界患者進行的一項研究中,只有 26% 的患者對治療“有反應”(這意味著他們的症狀在評定量表上至少下降了 50%),不到 13% 的患者處於12 個月末緩解。研究人員總結說,這些發現“揭示了非常低的反應和緩解率”。
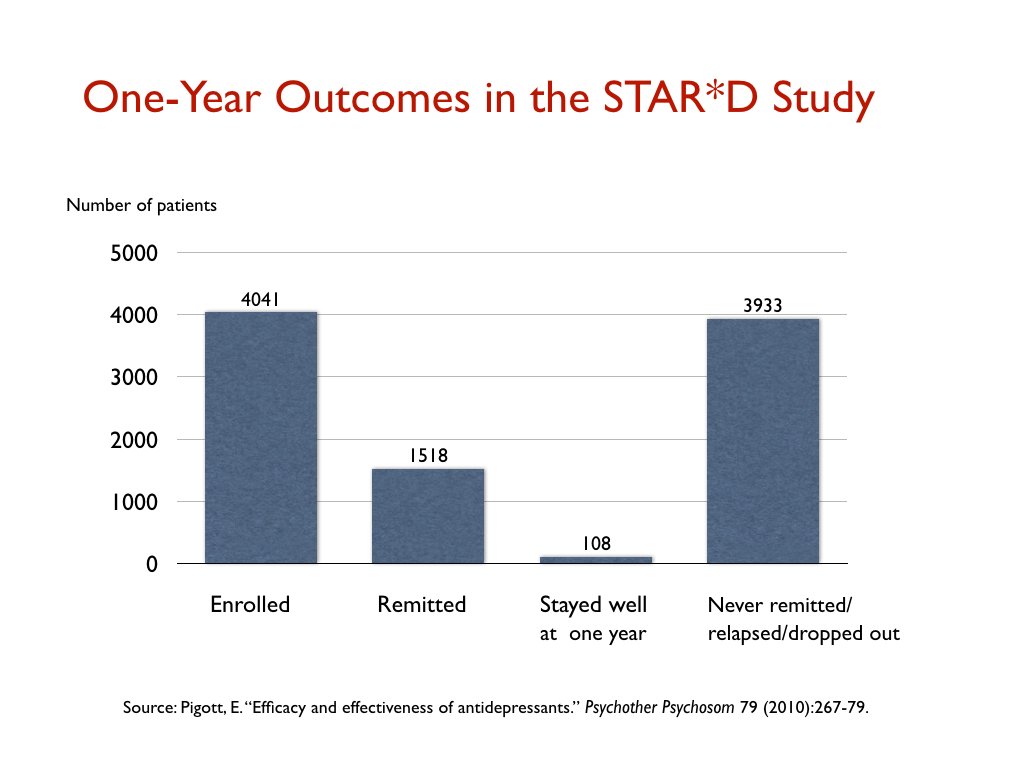
由 NIMH 資助的 STAR*D 試驗被譽為有史以來規模最大的抗抑鬱藥試驗,但在“現實世界”患者中產生了同樣糟糕的結果。參加試驗的 4,041 名患者接受了多達四項抗抑鬱藥試驗,以找到導致緩解(定義為漢密爾頓量表評分低於 7 分)的試驗,只有 38%的患者達到了這一水平的改善。
那些出院的人隨後會被帶入一項長期的後續研究,在那裡他們將獲得盡可能最好的臨床護理。然而,在一年結束時,參加 STAR*D 試驗的 4,041 名患者中只有 108 名患者病情好轉,並在試驗結束時保持良好狀態。其餘的人要么從未退還、復發或在某個時候退出。即一年保持良好率為 3%。
最近,一個國際研究小組在對 1,217 名被診斷患有重度抑鬱症的患者進行的一項研究中報告說,只有 24% 的人對抗抑鬱藥治療(單獨或與心理治療相結合)有反應。34% 是“非抗抑鬱藥的反應者”,而其餘 41% 的人表現如此糟糕,以至於他們被認為是“抗治療”。近 60% 的人最終服用了多種藥物,包括多種抗抑鬱藥、抗精神病藥、苯二氮卓類藥物和其他藥物組合。
這些真實世界的研究沒有安慰劑對照,因此沒有與未經治療的類似患者組進行比較。這就提出了一個明顯的問題:抑鬱症的自然過程是什麼?
在抗抑鬱藥時代之前,抑鬱症被認為是一種偶發性疾病,而不是一種慢性疾病。據說幾個月內自發恢復率超過50%,到一年年底這個恢復率達到85%左右。正如 NIMH 抑鬱症部門的負責人 Dean Schuyler 在 1974 年的一本書中所解釋的那樣,大多數抑鬱症發作“在沒有特別乾預的情況下幾乎完全康復而結束。” 12
然而,在引入抗抑鬱藥後,這種疾病開始變得更加慢性。在 1970 年代,幾位臨床醫生觀察到這種藥物正在導致疾病“慢性化”,隨後的流行病學研究證實,抑鬱症的長期病程已經發生了變化。APA 1999 年的教科書總結了新研究的結果:“只有 15% 的單相抑鬱症患者經歷過一次疾病發作”,而對於剩下的 85%,隨著每次新發作,緩解變得“不那麼完整和新復發會隨著更少的挑釁而發展。” 13
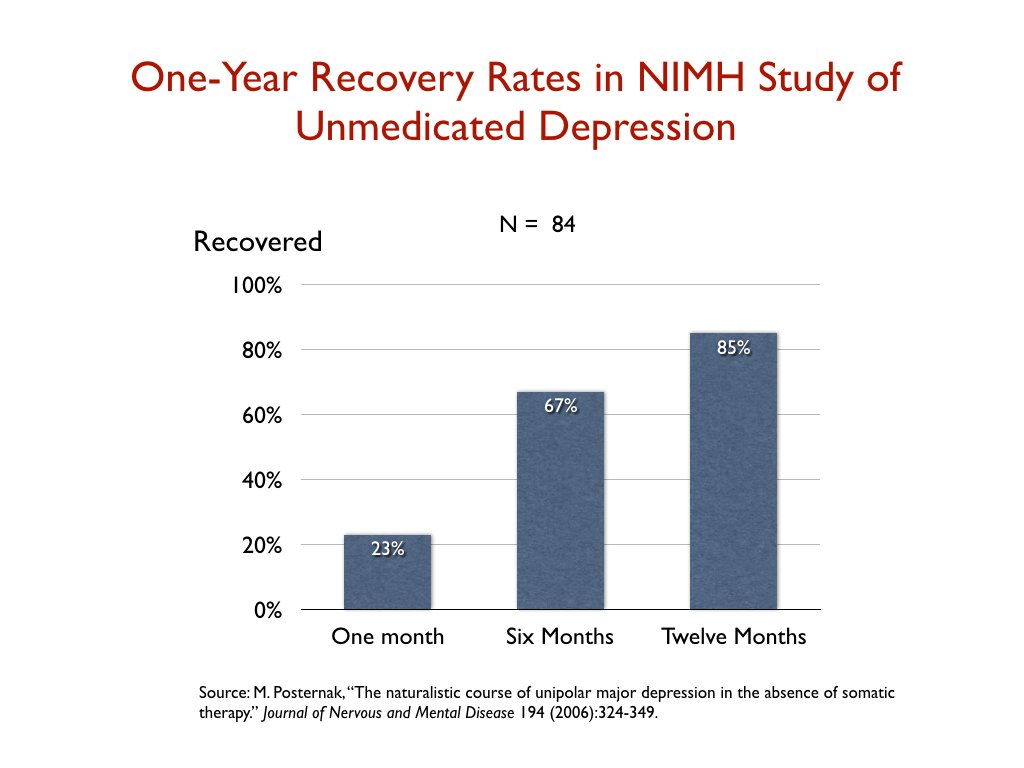
由於藥物治療患者的結果如此糟糕,NIMH 資助了一項研究,以評估現代“未經治療的抑鬱症”的過程。也許抑鬱症的自然過程已經改變?2006 年,研究人員報告說,23% 的未接受藥物治療的患者在一個月內康復;六個月內達到 67%;和 85% 在一年內。研究人員得出結論,這些結果與抗抑鬱藥前時代的結果相呼應。他們寫道:“如果多達 85% 的不接受軀體治療的抑鬱症患者在一年內自發康復,那麼任何干預措施都很難證明比這更好的結果。”
這就是從對現實世界患者的研究中得出的風險收益方程。也許 25% 的人會對抗抑鬱藥有反應,也許 15% 左右的人會對治療有反應並保持健康。也有理由相信,未經治療的患者的一年康復率遠高於此。
長期結果
行業資助的試驗在藥物六週結束時提供了風險收益方程。對現實世界患者的臨床研究提供了有關被診斷患有重度抑鬱症的人的百分比信息,這些人在較長時間(通常為六個月至一年)的研究中的某個時間點會對抗抑鬱藥產生反應並在結束時仍然很好的研究。需要評估的第三個問題是:接受抗抑鬱藥治療的患者在更長的時間(兩年或更長時間)中的表現如何?
這個問題可以追溯到長達一年的臨床研究中出現的問題:疾病的自然長期病程是什麼?為了使抗抑鬱藥長期有效,它需要提高自然恢復率。
不幸的是,有大量證據表明,總體而言,抗抑鬱藥會增加一個人患慢性抑鬱症和功能障礙的風險。我回顧了流行病解剖學中收集的證據;有關該研究的摘要,請參見Mad in America。
1990 年代中期,意大利精神病學家 Giovanni Fava 在一系列論文中提出了這一擔憂。他寫了:
“抑鬱症中的抗抑鬱藥物可能在短期內有益,但從長遠來看,通過增加對抑鬱症的生化易感性,會惡化疾病的進展。. . 使用抗抑鬱藥可能會使疾病發展為更惡性且治療無反應的過程。”
在他關於這個主題的文章中,法瓦指出,抗抑鬱藥會導致血清素系統發生與其預期效果相反的變化,並推斷這可能是大腦對抑鬱“敏感”的機制。
2012 年,美國精神科醫生、情緒障礙專家 Rif El-Mallakh 得出結論,SSRIs 可能導致慢性“遲發性煩躁不安”。他指出,在最初接受抗抑鬱藥治療的患者中,高達 40% 的患者最終會“產生耐藥性”,而繼續服用該藥物的患者中,高達 80% 的患者會出現症狀復發。
“長期暴露於強效血清素再攝取泵 (SSRIs) 拮抗劑的個體會出現慢性和難治性抑鬱狀態。由於這種慢性抑鬱狀態的發作延遲,它被稱為遲發性煩躁不安。遲發性煩躁症表現為一種慢性煩躁狀態,最初通過抗抑鬱藥物暫時緩解,但最終變得對抗抑鬱藥物無反應。5-羥色胺能抗抑鬱藥可能對遲發性煩躁症的發展特別重要。”
這就是抑鬱症患者——以及整個社會——在過去 30 多年中被告知的抗抑鬱藥與科學文獻中所講述的故事之間的差距。公眾被引導相信抗抑鬱藥修復了大腦中的化學失衡,因此可以被認為是導致抑鬱症的病理學的解毒劑,並且臨床研究表明這些藥物“有效”。事實上,研究文獻講述了以下故事:
- 抑鬱症不是由已知的大腦化學失衡引起的
- 抗抑鬱藥會導致大腦以一種與正常情況“質量和數量上都不同”的方式開始運作
- 在行業資助的試驗中,只有八分之一的患者可以說從治療中受益
- 對現實世界患者的研究發現,只有少數患者對抗抑鬱藥有反應,而在一年結束時仍然保持良好狀態的患者相對較少
- 接受治療的患者的長期結果特別差,有證據表明使用它們會增加一個人患慢性病的風險
當然,這些信息將使患者能夠就是否服用抗抑鬱藥做出明智的選擇。然而——這是 APA 如何繼續誤導公眾的一個例子——以下是 APA目前告訴公眾關於抗抑鬱藥療效的內容:
“80% 到 90% 的抑鬱症患者最終對治療反應良好。幾乎所有患者的症狀都得到了一些緩解。”
為什麼需要訴訟
所有社會都需要他們的醫學界向公眾提供關於疾病性質的已知信息以及治療該疾病的風險和益處的誠實信息。
抑鬱症的化學失衡故事違反了誠實的義務,而且非常嚴重。代替抑鬱症患者給予知情同意所需的信息,患者和公眾被告知了一個有利於行會利益和製藥公司經濟利益的虛假故事。從本質上講,營銷故事取代了科學故事。
Mad in America 發表了許多人的故事,這些人被告知大腦中的化學物質失衡,在服用抗抑鬱藥後,他們的生活崩潰和燃燒,很多人最終喝下了藥物雞尾酒。他們的故事剛剛開始暗示化學失衡欺騙所造成的巨大傷害。
然而,即使精神病學家說蒙克里夫的論文“沒有什麼新鮮事”,幾十年來也沒有公開承認以這種方式誤導患者和社會的不當行為或道歉。Carlat 在他對 NPR 的On Point節目的評論中,甚至在一定程度上證明了這一點,將其歸為一個善意的謊言。他說,有時需要向精神病患者提供有關“不完全準確”的精神藥物信息。
與此同時,APA 繼續宣傳,告訴公眾幾乎所有患者最終對抗抑鬱藥反應良好。這是一個虛偽的謊言,勝過抗抑鬱藥修復化學失衡的故事。
這就是為什麼需要集體訴訟的原因。在這一點上,那些促進遭受化學失衡的人並沒有為此付出任何代價。相反,錢已經賺了,事業已經光彩照人,而我們的社會一直在承擔成本。
集體訴訟將很好地服務於社會。它將強調醫生提供“知情同意”的法律義務,以及醫學學科向社會提供符合此標準的信息的法律義務。
***
資料來源:這裡敘述的大部分歷史和研究摘自流行病解剖:神奇子彈、精神病藥物和美國精神疾病的驚人上升,我在 2010 年出版的一本書,以及影響下的精神病學:制度腐敗,社會我與麗莎·科斯格羅夫(Lisa Cosgrove)合著的 一本書《傷害與改革處方》 ,於 2015 年出版。
- S.杜博夫斯基。“情緒障礙” ,精神病學教科書,由 R. Hales 編輯,第三版(華盛頓特區:美國精神病學出版社,1999 年):516。
- 正如 J. Lacasse 所引用的那樣。“血清素和抑鬱症:廣告和文獻之間的脫節。” 公共科學圖書館雜誌 2 (2005):1211-16。
- 正如 S. Kirk 所引用的,DSM 的銷售(霍桑,紐約:Aldine de Gruyter,1992):114。
- 參見Anatomy of an Epidemic,第 272-276 頁,全面了解這項公關工作。
- J.富蘭克林。“心靈修復者。” 巴爾的摩太陽報,1985 年 7 月出版的系列。
- 美聯社。“研究人員說,抑鬱症的治療可能即將到來。” 1981 年 10 月 12 日。
- N.安德烈森。破碎的大腦(紐約:Harper & Row,1984 年):29 -30、133。
- F.舒默。“再見,布魯斯。” 紐約,1989 年 12 月 18 日。
- G.考利。“百憂解:抑鬱症的突破性藥物。” 新聞周刊,1990 年 3 月 26 日。
- B.鄧肯。“揭露神話製造者。” 心理治療網絡, 2000 年 3 月/4 月。
- R. Harding,解開大腦的秘密。Family Circle雜誌,2001 年 11 月 20 日,第 61.
- D. 舒勒。抑鬱譜(紐約:傑森·阿倫森,1974 年):47。
- 精神病學教科書,同上,547。